There’s an expiration date on the “big box” model for medicine. Hospital bed counts in the U.S. have dwindled after decades of cost cutting—a capacity shortage that will hit hard as aging populations manage chronic conditions.
“The length of stay is increasing, acuity is increasing, and ultimately, it’s impacting the resources for the hospital,” says Kathleen Schwarz, director of healthcare consulting in HOK’s New York office.
By 2032, UCLA researchers predict that average hospital capacity in the U.S. could reach 85%—the widely accepted benchmark for a critical general bed shortage—likely causing medical errors and delayed emergency treatment.
With hospital staff already stretched thin, simply adding square footage to a centralized site isn’t a workable solution. “Clinical work is extremely challenging. Failure is not an option,” says Sarah Holton, a senior healthcare consultant for HOK in Tampa. “Considering the stress we’re under, we want to make sure the space facilitates our work.” To best distribute their available resources, health systems must extend beyond a single pinpoint on the map.
The Structural Shift: The Mothership
Expanded outpatient care isn’t just offsetting decreased inpatient capacity. It also gives health systems flexibility to meet their communities’ changing needs.
“The single greatest challenge facing our healthcare clients is uncertainty,” says Amine Khemakhem, firmwide director of Healthcare in HOK’s Los Angeles studio. “Trying to predict the future is a difficult thing.”
While managing costs and staffing shortages, health systems must also plan how they’ll use their facilities in the coming decades.
“Patient population needs have peaks and valleys,” Schwarz says. “Demographics continue to change.”
Aging populations with chronic conditions are driving a need for high-intensity ICU care, for example. Meanwhile, general medical-surgical units are seeing higher acuity patients than before, thus driving lower-acuity care to homes or alternate settings.
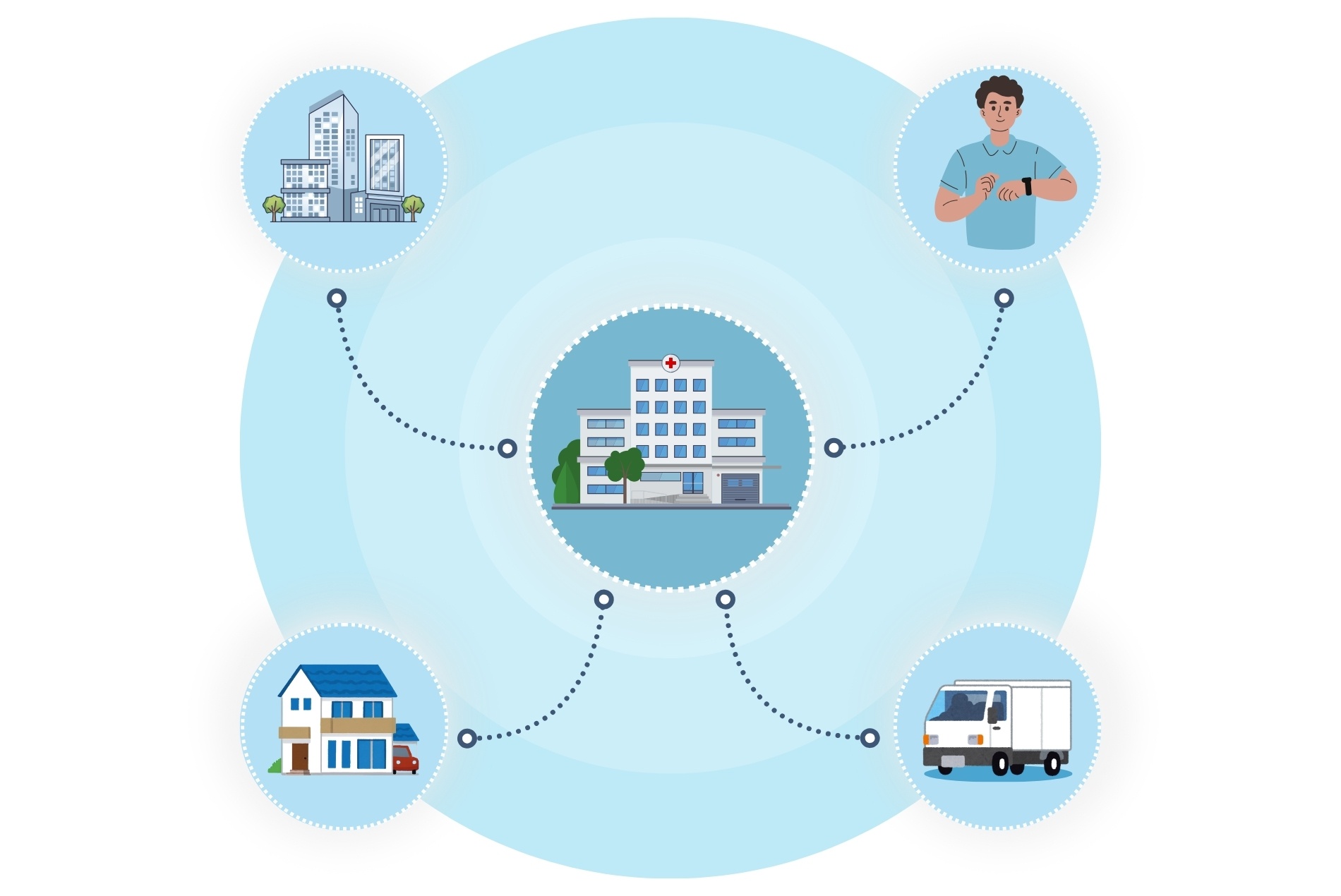
The solution is a hub-and-spoke model that transforms the physical hospital from a single location attempting to meet all a community’s needs into a mothership that houses complex care while dispersing routine care to satellite clinics and patients’ homes. This reduces travel time for patients and gives health systems flexibility to concentrate resources where and when they’re needed.
The Logistical Solution: Healthcare on Demand
Emerging home-care models suggest that the service is both in demand and scalable. In announcing a merger with fellow mobile healthcare provider Medically Home, DispatchHealth claimed “the combined organization could free up more than 62,000 bed days, easing strain on health systems while improving patient access to high-quality care at home.”
Cleveland Clinic’s Hospital Care at Home uses “a centralized command center staffed with nurses, physicians and pharmacists to provide around-the-clock virtual monitoring.” Nurses from this program reported closer connections with patients and noted the lowered risk of hospital-acquired infections.
“Most chronically ill patients prefer to have their care at home,” Schwarz says. “Getting out is not easy for them. If we can deliver care at home, it makes it that much more efficient and beneficial. And then our resources can remain at the hospital or acute sites.”
A survey by the University of Southern California Schaeffer Center confirms this preference among patients whose needs aren’t necessarily chronic: About half of respondents said they would prefer to receive hospital-level care at home, and most said they believe people recover more quickly there than at a hospital. Even the best-run hospitals can be chaotic environments, and care at home offers patients control over their surroundings.
“It’s about creating as much calm for the individual as possible so that the patient can really absorb what’s being communicated,” says Donald Cremers, senior project interior designer in HOK’s San Francisco studio.
An on-demand model gives patients more control while enabling providers to respond quickly as needs arise. An app integration, for example, could allow patients to request home care from trained mobile healthcare providers just as easily as calling an Uber.
The Universal Proof Point: Diversion
The logic of the hub-and-spoke model is mirrored in efforts to reshape the relationship between the justice system and behavioral healthcare; behavioral health interventions can divert individuals who might otherwise be on a path to a correctional institution.
“Diversion centers—community centers that can be resourced for the population that’s suffering from mental health instability and substance use disorders—would be a way to avoid the escalation of these problems to the correctional system,” says Shiva Mendez, Behavioral Health practice leader at HOK in San Francisco.
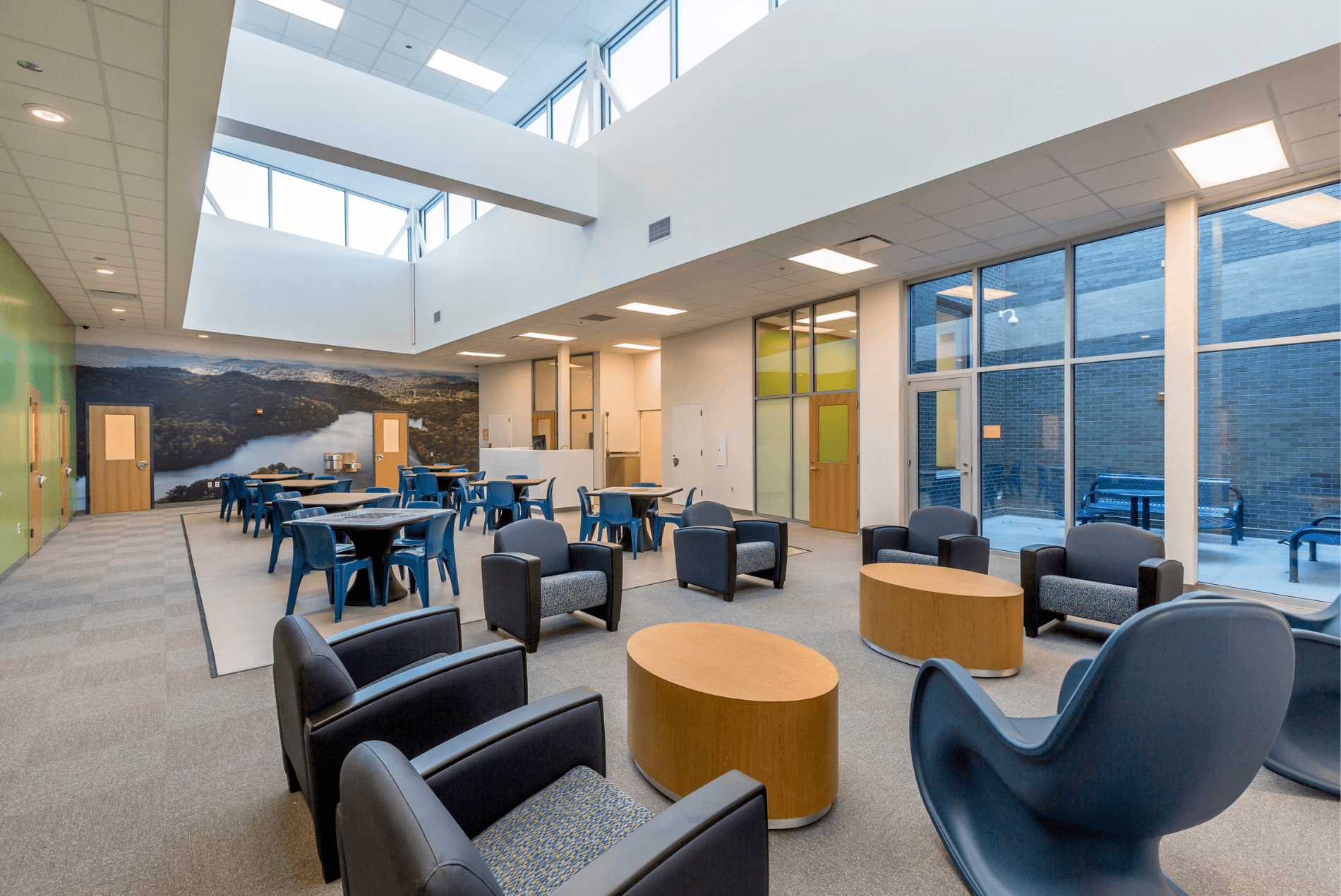
This vision shaped HOK’s design for downtown Nashville’s Davidson County Metro Criminal Justice Center (above). The center includes a 60-bed mental health and substance abuse treatment diversion unit, called the Behavioral Care Center, where individuals receive gender-responsive, trauma-informed care in a short-term residential setting. Residents who complete the program do not face criminal charges but are instead provided with resources for continued care. The Davidson County Sheriff’s Office reports that the BCC impacts up to 2,000 individuals annually.
Just as specialized treatment facilities can divert mental health patients from correctional institutions, personalized home care can divert patients from hospitals.
The Infrastructure: Invisible Data
Chronic conditions demand significant resources—not just due to their longevity, but because they often come with comorbidities.
“A lot of chronically ill patients are managing more than one disease at a time,” Schwarz says, citing diabetes and hypertension as examples of diagnoses that often appear in tandem. Monitoring all comorbidities at once offers providers a comprehensive look at the patient’s health, she says, and can help prevent the need for a trip to the hospital.
Wearable devices that track chronic conditions can streamline treatment and serve as a preventive tool, giving providers real-time insight into their patients’ well-being. Many consumer-facing wearables, such as smartwatches from Apple and Google, have FDA-cleared features for biometric monitoring.
“I like to think that, with devices that link us back to our caregiver, that they will know us more fully,” says Mark Banholzer, senior project designer in HOK’s Chicago studio. “Wouldn’t it be nice if my whole life story became part of my medical record? And because of that, clinical decisions are broader and maybe have a greater impact?”
Advances in AI and data processing are making wearables increasingly viable for hospital-at-home models. A report by Johns Hopkins University School of Medicine and the Scripps Research Translational Institute acknowledges that turning wearable data into clinically actionable insight remains a challenge, but argues that large language models now have the computing power to automate the process.
Beyond remote monitoring, wearable data could enhance inpatient care, too. Banholzer suggests, for example, that a wearable could connect to a patient’s hospital room to adjust to their environmental preferences, such as temperature and color of lighting, and help ease anxiety.

The Vision
In the face of a looming bed shortage, healthcare needs a new model. Tech solutions can ease the transition.
Allison Wagner, regional leader of Healthcare for HOK in London, cites banking as an industry that saw a drastic transformation from a destination into a distributed service thanks to new technologies: “We see how AI has worked in the banking industry. We never go to a bank anymore; we just go on our apps. Nowadays, with what’s happening with healthcare and wearables and apps, it’s completely changing how healthcare will be delivered and how we design hospitals in the future.”
The result: care that meets patients exactly where they are.
Continue the Conversation
To learn more about how these insights can apply to your health system, reach out to our team:
Amine Khemakhem, Firmwide Director of Healthcare, Los Angeles | amine.khemakhem@hok.com
Kathleen Schwarz, Director of Healthcare Consulting, New York | kathleen.schwarz@hok.com
Allison Wagner, Regional Leader of Healthcare, London | allison.wagner@hok.com
Sarah Holton, Senior Healthcare Consultant, Tampa | sarah.holton@hok.com
Shiva Mendez, Behavioral Health Practice Leader, San Francisco | shiva.mendez@hok.com
Donald Cremers, Senior Project Interior Designer, San Francisco | donald.cremers@hok.com
Mark Banholzer, Senior Project Designer, Seattle | mark.banholzer@hok.com